Z. G. Hashmi1, S. Zafar2, T. Genuit1, E. R. Haut4, D. T. Efron4, J. Havens3, Z. Cooper3, A. Salim3, E. E. Cornwell III2, A. H. Haider3 1Sinai Hospital Of Baltimore,Department Of Surgery,Baltimore, MD, USA 2Howard University Hospital,Department Of Surgery,Washington, DC, USA 3Brigham And Women’s Hospital,Department Of Surgery,Boston, MA, USA 4Johns Hopkins University School Of Medicine,Department Of Surgery,Baltimore, MD, USA
Introduction: Nationwide efforts at trauma quality improvement aim to reduce in-hospital trauma mortality. However, the magnitude of this mortality reduction at the national level remains largely unknown. Our objective was to determine a nationwide estimate of number of lives that could potentially be saved if high-mortality trauma centers improved their performance.
Methods: Adults with blunt/penetrating injuries included in the Nationwide Emergency Department Sample 2006-2010 were analyzed. Hospitals were classified as high, average or low-performers based on risk-adjusted in-hospital mortality using the standardized Trauma Quality Improvement Program (TQIP) benchmarking methodology. Generalized linear modeling, adjusting for demographics and injury severity characteristics, was then used to estimate the relative-risk of death for patients treated at high/average performing hospitals versus low-performing centers. Subsequently, weighted national estimates of preventable mortality were determined for each of the following; 1)Conservative model: low-performing hospitals improve to average-performing, 2)Intermediate model: low-performing hospitals improve to average and average improve to high-performing and 3)Best-case model: all hospitals improve to high-performing.
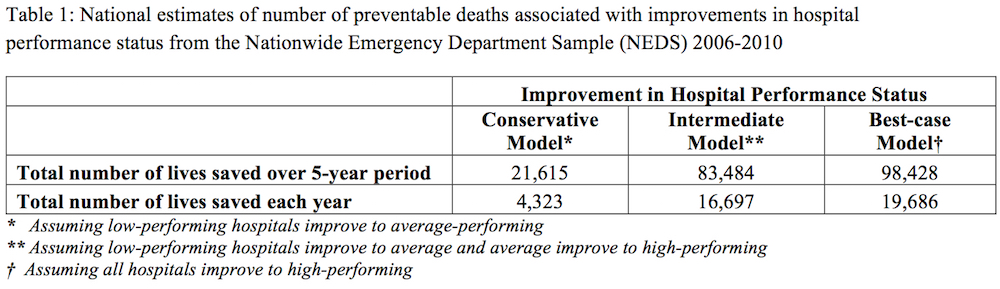
Results: A total of 9,992,202 trauma patients from 1771 hospitals were included. 151 (8.5%) hospitals were classified as high-performing, 1,506 (85.0%) as average and 114 (6.4%) as low-performing. For conservative and intermediate models, an estimated 4,323 and 16,697 trauma deaths, respectively, could be prevented annually. Additionally, if all hospitals were to deliver the highest quality of care, an estimated 19,686 lives could potentially be saved each year.
Conclusion: If all trauma centers achieved outcomes similar to those at the highest-performing centers, nearly 100,000 lives could be saved over 5 years. These national estimates demonstrate the tremendous societal benefits associated with provisioning high quality of trauma care. Concerted efforts aimed at the standardization and implementation of high quality trauma care should therefore be a priority.