K. P. Kulkarni3, R. S. Chamberlain1,2,3 1Saint Barnabas Medical Center,Surgery,Livingston, NJ, USA 2New Jersey Medical School,Surgery,Newark, NJ, USA 3St. George’s University School Of Medicine,St. George’s, St. George’s, Grenada
PURPOSE: Optimal glycemic control in cardiac surgery patients remains a laudable but confusing practice. Existing studies have primarily employed two maintenance strategies using either tight glycemic control (maintain <120 mg/dl) or liberal control (<200 mg/dl) with conflicting outcomes. Meta-analysis and meta-regression were performed to better delineate which approach (if any) is associated with reduced perioperative morbidity and/or mortality.
Methods: A comprehensive literature search of PubMed, Google Scholar and the Cochrane Central Registry of Controlled Trials was completed. Keywords searched were ‘insulin’,‘bypass’,’coronary’,’CABG’,’glucose’,’artery’,’intensive’,’cardiac’, and ‘surgery’. Eligible studies were randomized control trials (RCTs) utilizing two different glycemic control strategies with a mortality outcome. Primary outcomes were mortality, intensive care unit (ICU) length of stay (LOS), and hospital LOS.
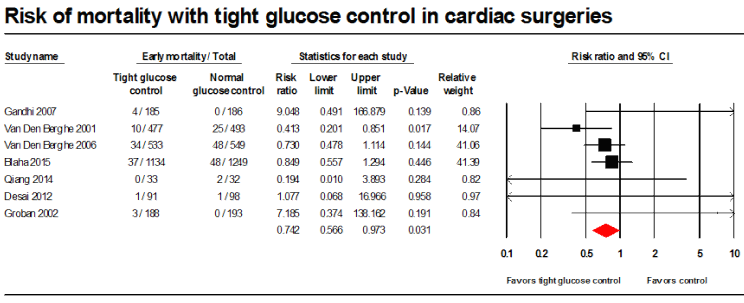
Results: 14 studies were included in this study. Intensive glucose control significantly reduced mortality (relative risk (RR) = 0.742, 95% CI=0.566 to 0.973; p=0.031) and ICU LOS (Standardized difference of mean (SDM) = -0.352, 95% CI=-0.352 to -0.692; p=0.042) but did not influence overall hospital LOS (SDM= -0.255, 95% CI = -0.722 to 0.211; p=0.283). Significant secondary outcomes were overall infection (RR=0.444, 95% CI=0.322 to 0.611; p<0.001) and atrial fibrillation rates (RR=0.722, 95% CI=0.582 to 0.896; p=0.003). No difference in stroke (RR=2.279, 95% CI=0.525 to 9.885; p=0.271), deep sternal infection (RR=0.599, 95% CI=0.242 to 1.484; p=0.268), acute renal failure (RR=1.337, 95% CI=0.468 to 3.821; p=0.588), or prolonged intubation rates were observed (RR=0.990, 95% CI=0.661 to 1.483; p=0.962).
Conclusion: Optimal glycemic control is significantly linked to improved perioperative outcomes in cardiac surgery patients. Intensive glucose control (< 120 mg/dl) reduces mortality and ICU LOS in cardiac surgery patients, while also decreasing overall postoperative infection and atrial fibrillation rates compared to more liberal glycemic strategies. Additional adequately powered studies are needed to further investigate the nuances of optimal intensity and duration of glycemic control in this patient population.