C. S. Lau1,3, R. S. Chamberlain1,2,3 1Saint Barnabas Medical Center,Surgery,Livingston, NJ, USA 2New Jersey Medical School,Surgery,Newark, NJ, USA 3Saint George’s University,Grenada, Grenada, Grenada
Introduction: Real-time ultrasound guidance for central venous catheter (CVC) insertion has been shown to increase cannulation success rates and reduce complications in adults. Literature regarding ultrasound guided CVC placement in children remains limited and conflicting. This meta-analysis examines the impact of ultrasound guided CVC placement among pediatric patients in regards to success rate, number of attempts required, incidence of accidental carotid artery puncture, and time to cannulation.
Methods: A comprehensive literature search of all published randomized control trials (RCTs) assessing the use of real-time ultrasound guided CVC insertion in pediatric patients <18 years of age was conducted using PubMed, Cochrane Central Registry of Controlled Trials, and Google Scholar (1966-2015). Keywords searched included ‘ultrasound guided’ and ‘central venous catheter’. Studies comparing the use of real-time ultrasound CVC insertion with anatomic landmark CVC placement in pediatric patients <18 years of age were included. Primary outcomes analyzed were cannulation success rate, number of attempts required, incidence of carotid artery puncture, and time to cannulation.
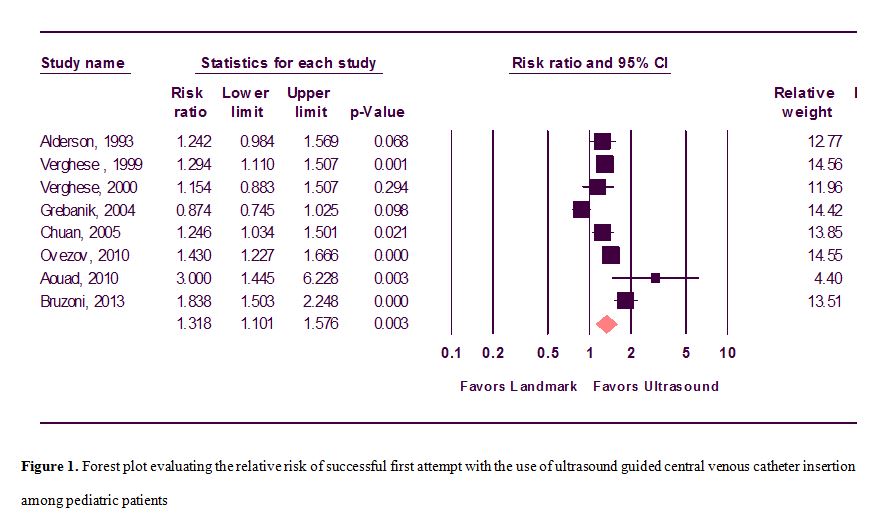
Results: 8 RCTs involving 760 patients (367 via ultrasound guidance and 393 via anatomic landmark placement) were analyzed. Ultrasound guided CVC insertion significantly increased success rates by 31.8% (Relative Risk (RR) = 1.318; 95% CI, 1.101 – 1.576; p=0.003) and decreased the mean number of attempts required (Mean Difference (MD) = -1.261; 95% CI, -1.711 to -0.812; p<0.001). A trend towards a decrease in the risk of accidental carotid artery puncture with the use of ultrasound guided CVC insertion was also observed (RR = 0.359; 95% CI, 0.118 – 1.093; p=0.071). Ultrasound guided CVC insertion was not associated with a significantly longer time to CVC placement (MD = 1.175 = -0.287 to 2.636; p=0.115).
Conclusion: Ultrasound guided CVC placement is associated with significantly higher success rates and decreased mean number of attempts required for cannulation. There is also a trend towards a decrease in accidental carotid artery puncture, which was not statistically significant likely due to inadequate sample size. Ultrasound guided CVC insertion improves success rates, efficacy, and safety among pediatric patients. Additional studies are required to determine the efficacy and safety of ultrasound guided CVC insertion in specific age populations of neonates compared to older children, and in the various healthcare settings.