C. Kapsalis1, A. Lai1, D. Kim1, D. Ciesla1 1University Of South Florida College Of Medicine,Tampa, FL, USA
Introduction:
Trauma center standards define the resources and processes that best meet the needs of injured patients. The regional trauma system aims to match the distribution and level of designated trauma centers to meet the needs of its population. Population demographics vary substantially across regions and predict variation in trauma center demographics. The purpose of this study was to characterize the variation in Florida trauma center patient populations.
Methods:
A statewide discharge dataset was queried for all injury related discharges from Florida acute care hospitals using ICD-9 codes in 2014. Hospitals were categorized as non-trauma centers (NTC), Level 2 (DTC2), pediatric Level 2 (DTC2p), and Level I (DTC1) Designated trauma centers. Elderly patients with isolated hip fractures from falls were excluded. ICISS values were calculated for all ages based on survival risk ratios of the adult (age 16-65) age group for the 5 years preceding the reported year. An ICISS <0.85 defined high mortality risk and predicts <85% survival.
Results:
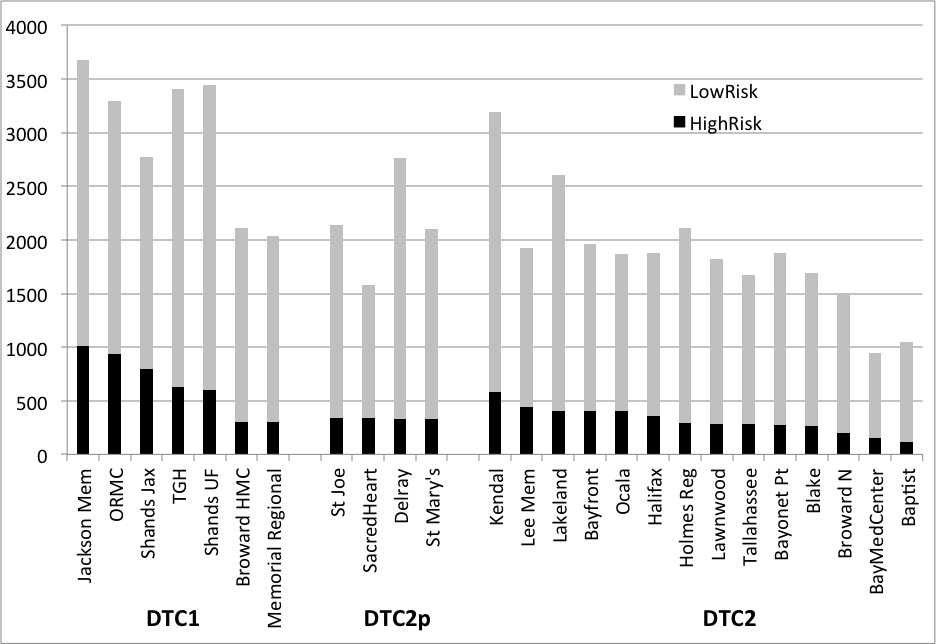
There were 133710 injured patients discharged from 211 Florida acute care hospitals in 2014; 54,478 (41%) from one of 24 designated trauma centers including 10226 (80%) of 12771 high-risk patients. Individual trauma center volumes are shown in the figure. Although there was variability within each group, DTC1’s as a group had a higher proportion of high risk patients (22%) compared to DTC2p (16%) and DTC2 (17%), lower proportion of elderly patients (26%) compared to DTC2p (42%) and DTC2 (43%), and a lower proportion of injuries resulting from falls (35%) compared to DTC2p (48%) and DTC2 (47%). Among the high risk patients, DTC1 treated a lower proportion of patients with Traumatic brain injuries (19%) compared to DTC2p (23) and DTC2 (28%).
Conclusion:
Although all trauma centers may meet level specific standards and serve distinct populations, there is significant variability in populations served among Level 1 and Level 2 trauma centers and substantial overlap between some Level 1 and Level 2 centers. This information is useful in trauma systems planning when designating trauma centers within specific regions.