G. E. Mendoza-Barrera1, W. Sanchez2, S. R. Brown1, A. Person1, D. Keleny1, D. Rigg1, M. Dale1, J. Dabestani1, D. K. Agrawal1, J. A. Asensio1 1Creighton University Medical Center,Surgery,Omaha, NE, USA 2Colombian Military Hospital,Nueva Granada Military School Of Medicine,Bogota, BOGOTA, Colombia
Introduction: Recent military conflicts have changed from more conventional to guerrilla and counter insurgency warfare with the subsequent refinement of newer antipersonnel devices such as improvised explosive devices (IEDs). The Iraq and Afghanistan conflicts have shown newer injury patterns with a subsequent decrease in definitive extremity vascular injury repairs, along with a significant increase in single and multiple limb amputations. Objectives of this study are to analyze the Colombian military experience with combat related extremity vascular injuries. Describe distribution of wounds, mechanisms of injury related to vascular injuries incurred in combat. Identify predictors of outcomes and validate conventional wounding patterns.
Methods: Retrospective review of 13 year prospective data base. Statistical analysis: Chi square, T test, ANOVA and stepwise logistic regression which included mode of injury (MOI), MOI over time, ISS, RTS, type of vascular injury, time to definitive surgical care, procedures performed, incidence of amputation and mortality.
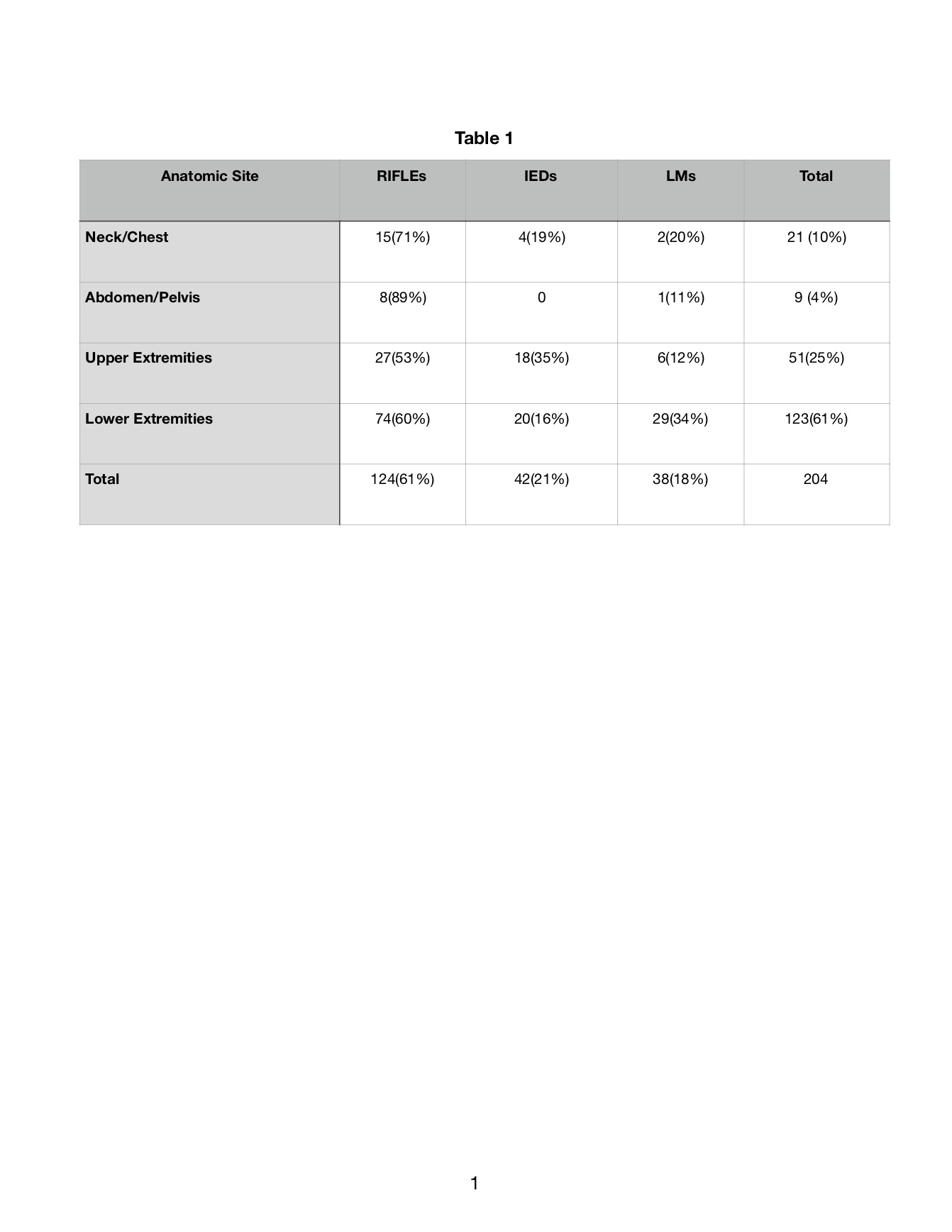
Results: 204 patients sustained 390 vascular injuries 159 (40.8%) arterial and 231(59.2%) . Weapons: Automatic Rifles (RIF) n=124 (60.7%), Improvised Explosive Devices (IEDs) n=42 (20.7%) and Land Mines (LMs) n=38 (18.6%). 70 patients (36.8%) were directly transferred from the field and 134 (63.2%) from MASH units. Mode of injury (MOI) remained unchanged. Extremity vascular injuries accounted for 86%: – 61% upper and 25% lower. Neck 10% , abdominal injuries 4%. 20 patients (9.8%) required amputation (19 LE and 1 UE). Amputation was independent of MOI – RIF 9.7%, IEDs 13.1% and LM 9.8%, – p < 0.05. Amputation was dependent on presence of combined arterial-venous injuries (AVI), ligation of a named vein and performance of fasciotomy. 11/20 (55%) with lower extremity amputations sustained arterial-venous (AV) injuries, popliteal vessel injury managed with arterial interposition vein graft and popliteal vein ligation. Overall mortality 3.9% (8/204).
Conclusion: For combatants sustaining vascular injuries automatic rifles remain responsible for majority of these injuries. Extremity vascular injuries are as in other wars most prevalent. Strategies to decrease the rate of amputation for popliteal artery injuries: avoid ligation of popliteal vein and perform complete fasciotomy. Trauma surgeons must remain adept at vascular injuries management.