T. A. MacArthur2, M. Auton3, A. Tischer3, J. Dong4, R. A. Kozar5, J. Goswami2, M. S. Park1 1Mayo Clinic,Department Of Surgery, Division Of Trauma, Critical Care And General Surgery,Rochester, MN, USA 2Mayo Clinic,Department Of Surgery,Rochester, MN, USA 3Mayo Clinic,Division Of Hematology, Department Of Medicine,Rochester, MN, USA 4University Of Washington,Hematology Division, Department Of Medicine, Member- Bloodworks Research Institute,Seattle, WA, USA 5University Of Maryland,Department Of Surgery,Baltimore, MD, USA
Introduction: Von Willebrand factor (VWF) is synthesized in megakaryocytes and endothelial cells (EC) as a single-chain propolypeptide that consists of repeat domains of D1-D2-D’-D3-A1-A2-A3-D4-C(1-6)-CK. After synthesis, VWF multimers are either released constitutively into circulation or stored in granules of ECs and platelets, where they form ultra-large (UL)VWF multimers. Under physiologic conditions, ULVWF is rapidly cleaved by the metalloprotease ADAMTS-13, up release, to generate the smaller plasma forms of VWF multimers found in circulation. This cleavage prevents spontaneous pro-thrombotic VWF-platelet interaction in circulation while maintaining the hemostatic activity of VWF at the site of vascular injury. After trauma, ULVWF multimers are released as part of the acute phase reaction. When ULVWF release overwhelms the proteolytic capacity of ADAMTS-13 this safeguard is bypassed, potentially contributing to the coagulopathy of trauma.
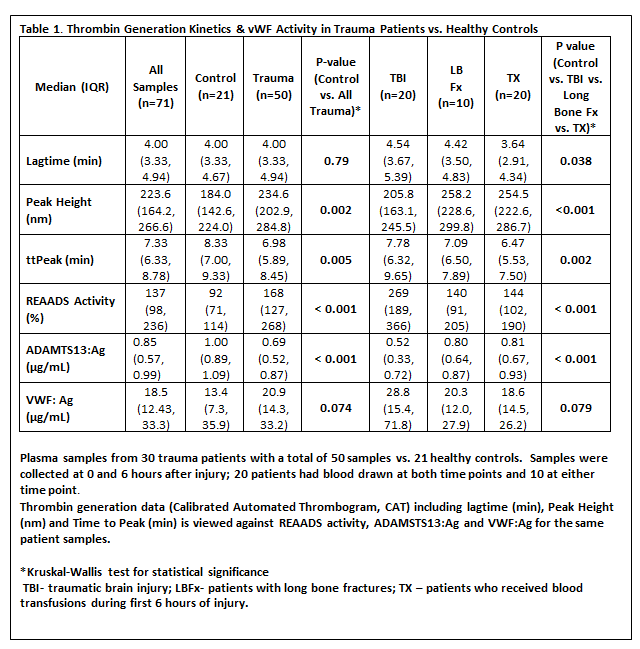
Methods: Fifty plasma samples from 30 trauma patients were evaluated and compared to 21 healthy volunteers. The patients were stratified by injury type including traumatic brain injury (TBI), Long Bone Fracture (LBFx) and need for any blood transfusion (TX). We assessed the plasma concentrations of VWF:Ag and ADAMTS-13:Ag, and the Rapid Enzyme Assays for Autoimmune Diseases (REAADS) activity of VWF, which measures the binding of a monoclonal antibody to an exposed epitope in the A1 domain. Kruskal- Wallis test for significance was performed on all subgroups, and results are presented in Table 1 against previously obtained thrombin generation data for the same patients.
Results: As compared to healthy volunteers, thrombin generation is enhanced in trauma patients, especially those that required any blood transfusion (Table 1). In all trauma patients, the VWF:Ag levels were elevated relative to controls. In addition, the REAADs activity was greater, especially in those with TBI. ADAMTS-13:Ag levels were also moderately reduced in all trauma patients, and this was most apparent in those with TBI.
Conclusion: These data demonstrate that trauma patients, especially those with TBI, have enhanced exposure of the VWF A1 domain (activated VWF) based on increased REAADS activity. The increase in REAADS activity coupled with the decrease in free plasma ADAMTS-13:Ag in all trauma patients, may indicate that ADAMTS-13 is not efficiently cleaving ULVWFs in these patients. Further investigation with a larger cohort is merited to assess whether VWF has any clinical significance in Trauma-induced Coagulopathy, such as in the development of venous thromboembolism.