S. A. Negash1, T. N. Mammo1, B. Ayele5, E. Anberber1, N. Starr4, T. G. Weiser2, 3 1Addis Ababa University, Surgery, Addis Ababa, ADDIS ABABA, Ethiopia 2University of Edinburgh, Surgery, Edinburgh, SCOTLAND, United Kingdom 3Stanford University, Surgery, Palo Alto, CA, USA 4University Of California – San Francisco, Surgery, San Francisco, CA, USA 5Addis Ababa University, Anesthesia, Addis Ababa, ADDIS ABABA, Ethiopia
Introduction: The operating theatre is one of the most expensive areas of a hospital, requiring large capital and recurring investments, and necessitating efficient throughput to reduce costs per patient encounter. On top of increasing costs, inefficient utilization of operating theaters results in prolonged waiting lists, high rate of cancellation, frustration of OT personnel as well as increased anxiety that negatively impacts the health of patients. This problem is magnified in developing countries, where there is a high unmet surgical need. However, no system currently exists to assess operating theatre utilization in Ethiopia.
Methods: A prospective study was conducted over a period of 2 months (May-June 2018) at our hospital. It is the largest hospital in the country and has the highest number of operating theaters. Surgical case start time, end time, room turnover time, cancellations and reason for cancellation were observed to evaluate the efficiency of eight operating theaters.
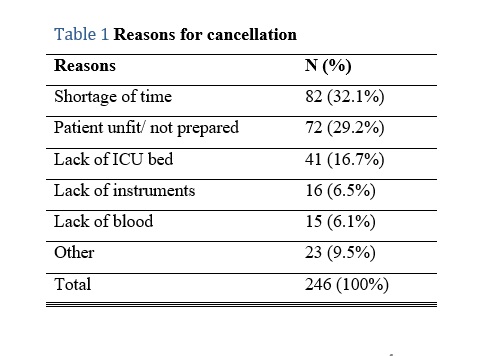
Results: A total of 933 elective procedures were scheduled during the study period. Of these, 246 were cancelled, yielding a cancellation rate of 35.8%. The most common reasons for cancellation were related to patient preparation (29.2%) and shortage of time (32.1%). Lack of facilities accounted for 29.3% of cancellations. Start time was delayed in 93.4% of cases (mean 8:56 am + 52 min). First case completion time was early in 47.9 % and delayed in 20.6% (mean 2:54pm + 156min). Turnover time was prolonged in 34.5% (mean 25 min + 49 min). Total operating theater utilization ranged from 10.5% to 174%. Operating theaters were underutilized in 42.7% while overutilization was found in 14.6%.
Conclusion: We found a high cancellation rate, most of which are avoidable. The most common reason was shortage of time which could be associated with overbooking or inappropriate use of time due to other delays. Turnover time was longer than average, however, intervention in this area would likely not make an impact on efficiency as number of procedures per OT each day is low. Other measured causes of poor efficiency included late start of the first case and variable (very early or late) end of the last case. We recommend future quality improvement projects focusing on these two areas to increase OT efficiency.