C. H. Lee1, R. Mabeza1, M. Park1, N. Chervu1, J. Hadaya1, K. Darbinian1, P. Benharash2 1David Geffen School Of Medicine, University Of California At Los Angeles, Surgery, Los Angeles, CA, USA 2David Geffen School Of Medicine, University Of California At Los Angeles, Cardiothoracic Surgery, Los Angeles, CA, USA
Introduction:
The Modified 5-point Frailty Index (mFI) has been incorporated in the National Surgical Quality Improvement Program (NSQIP) datasets as a means of identifying this condition in surgical patients. As frailty and colonic diverticular disease are both associated with advancing age, the study aimed to characterize the association of mFI score with clinical outcomes following colonic resections for diverticular disease.
Methods:
Adults (≥18 years) undergoing elective colon resection for diverticular disease were identified using the 2017-2019 NSQIP data reports. Subjects were assigned a point for each select comorbidity and grouped into 3 cohorts (mFI: 0, 1, >1). Prolonged length of stay (LOS) was defined as hospitalization longer than 95th percentile for the entire group. Multivariable regression analyses were used to examine the association of frailty with perioperative complications, unplanned reoperation, prolonged LOS, and 30-day readmissions.
Results:
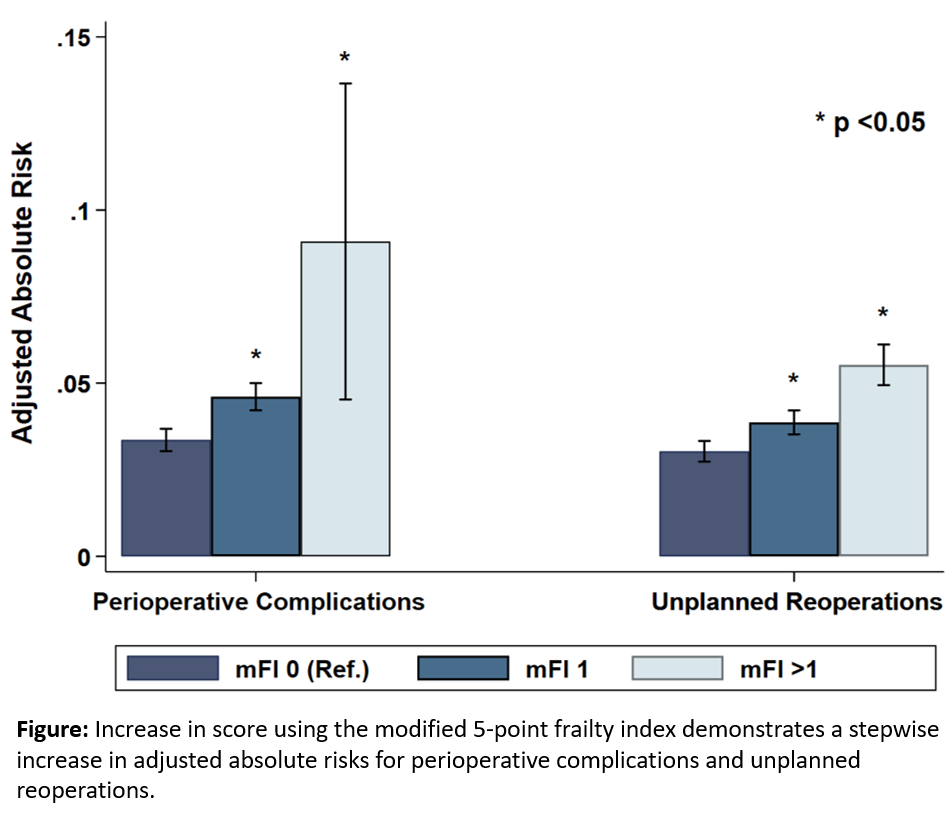
Among 22,675 surgical patients with diverticular disease who met study criteria, 47% were in the mFI-1 and 1% in the mFI>1 group. Subjects with a mFI≥1 less frequently underwent laparoscopic vs open resection (75 vs 80%, p<0.001) and more likely to undergo colonic resection with stoma formation (7.1% vs 4.7%, p<0.001) compared to the mFI-0 group. Despite these differences, the operative times were similar among the mFI-0 and mFI≥1 groups (201±86 vs 191±81 minutes, p<0.001). After adjustment, frailty was associated with increased odds of perioperative complications and unplanned reoperation (Figure). With mFI-0 as reference, with each increase in mFI score groups, the odds for a prolonged LOS after the operation increased in a stepwise fashion (AOR 1.25 and 3.55, p<0.01) as did 30-day readmissions (AOR 1.26 and 1.74, p<0.05).
Conclusion:
With nearly half of patients undergoing colonic resections for diverticulitis carrying frailty defining comorbidities, this condition is associated with increased risk of complications, prolonged index hospitalization and 30-day readmissions. Preoperative assessment of frailty using the mFI may improve shared decision making and focus quality improvement efforts on this vulnerable cohort.